Longevity Medicine - Is It The Health Revolution We So Desperately Need?
Explore the rapid evolution from the COVID-19 healthcare crisis to the current boom in longevity medicine. Highlighting the surge in investment and interest in anti-aging therapies, delve into the pro
Longevity Medicine - Is It The Health Revolution We So Desperately Need?
HILLARY LIN
APRIL 30, 2024
Just four short years (and an eternity) ago, we saw the near-collapse of our healthcare system. The COVID pandemic in 2020 resulted in four-hour-long ambulance waits in NYC, reopening of mass graves such as Hart Island, and $202.6B lost by the US health system.
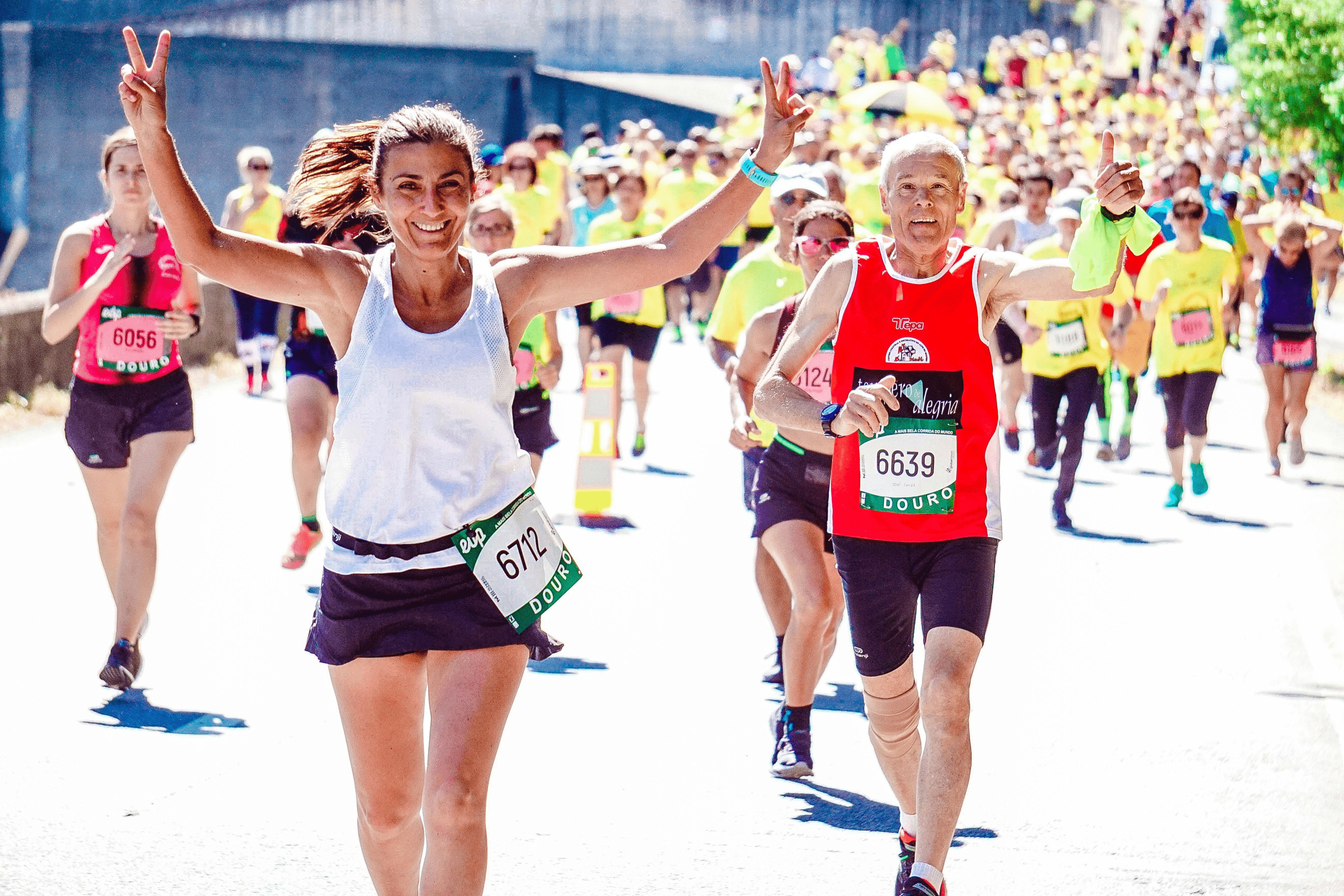
Fast forward to now, and a casual observer might get whiplash. Longevity is having a bit of a moment. From Peter Attia’s Outlive to a Longevity Castle in SF, we have turned 180 degrees from the crisis of the deep pandemic era to an age turned toward hope, health, and eternal youth.

Investors are excited, with VC funds dedicated to aging research and longevity startups already raising > $850M. The longevity and anti-aging therapy market is already valued at $27B, with some analysts believing the market will be worth far more - at least $600B - by 2025.
When did the Longevity Wave Begin?
As a medical doctor and startup founder, I have been puzzling over the change in the atmosphere. I was low-key obsessed with longevity even in my teens, before I (or anyone) knew much about human longevity. My first high school research projectinvolved working with Sir2 - a family of proteins made famous by longevity scientist David Sinclair’s lifespan research at Harvard.
The healthcare industry has tried out as many trends as a fashionista over the last couple decades. Digital health was the first attempt to bring healthcare anywhere close to the 21st century. Then there were sub-movements (or marketing buzzwords) promoting wellness, personalized medicine, value-based care, wearables, big data, and of course AI.

But in 2023 and 2024, we have seen a near explosion of interest in the field of longevity. After attending a powerhouse gathering of longevity physicians (held in NYC the past week by Longevity Docs), I’m feeling ever more curious and optimistic about the movement.
Is Longevity Medicine = Good Medicine?
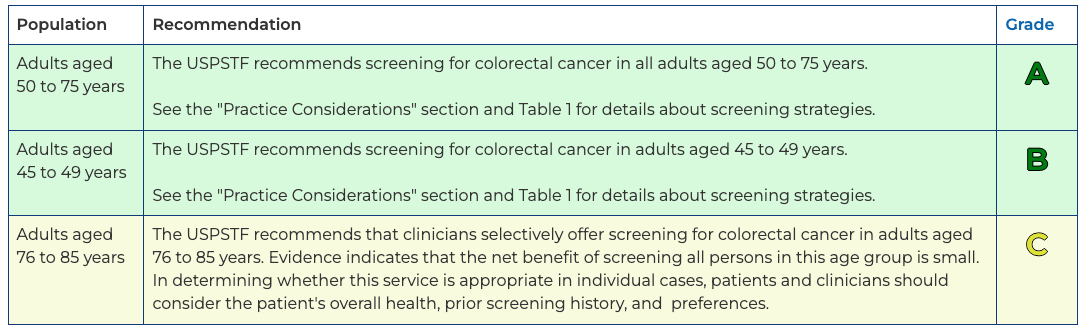
One of the countless polarizing spectra of modern medicine is between population health and individual treatment. On the one end, we need to conduct large-scale studies to prove certain interventions should be guidelines for wide swaths of the population.
View this post on Instagram
Fasting for Health and Longevity:
Unlocking the Power of Metabolic Rejuvenation
Read articleSecret to Longevity?
Part 1 of the VO2 Max Series
Read article
https://hillarylinmd.com
Unsubscribe · Preferences
The Longevity Letter
A weekly read on tests, treatment, and claims.
New issues look at what the evidence supports, what is premature, and what to skip.