Why I prescribe Rapamycin - but not to most of my patients
Discover why 2026 research has shifted Rapamycin from a "cellular cleanup crew" to a powerful shield for your DNA.
Hi ,
We've been prescribing Rapamycin in longevity medicine for years. The pitch was always the same: it triggers autophagy — your cells' internal cleanup crew — clearing out damaged proteins and dysfunctional organelles.
But a 2026 paper out of Oxford just changed our understanding entirely.
Researchers exposed human T-cells to DNA-damaging agents — the kind we get from UV light, metabolic stress, and basically living on Earth.
The cells pre-treated with Rapamycin didn't just survive better. They had significantly lower DNA damage burdens and double the survival rate.
Rapamycin wasn't just cleaning the house. It was reinforcing the foundation.
If Rapamycin can function as a DNA shield — not just a cellular cleanup broom — then the risk-benefit conversation shifts for a lot of patients. So this week, I'm doing a full deep dive: what we know, what's new, and exactly how I prescribe it in my clinic.
Let's look at the data.
The TL;DR:
- 🛡️ The Evidence: Six human trials that moved Rapamycin from "promising in mice" to "demonstrable in humans" — immune rejuvenation, muscle preservation, skin repair, ovarian protection, energy restoration, and now DNA shielding.
- 📋 The Protocol: The exact dosing strategy I use in my clinic — the safety on-ramp, the lean-mass-based targeting, the absorption rules that make or break the protocol, and the biomarkers I monitor.
- ⚡ Quick Hits: The upstream driver rapamycin can't touch (ER-phagy), why worrying about aging literally ages you, and the "living drug" capsule that could deliver longevity drugs in your body 24/7.
🧬 Why Rapamycin for Longevity?
Rapamycin has been the darling of the longevity world. It extends life in yeast, worms, flies, and rodents by 20-30%. It has shown efficacy in models of cancer, Alzheimer’s, mitochondrial disease, and progeria.
But we lacked the definitive human data to prove it wasn’t just a quirk of animal biology.
That changed with the seminal work by Dr. Joan Mannick and subsequent trials. We now have evidence that Rapamycin isn’t just slowing a theoretical “aging clock”—it is actively preserving the specific tissues that define our quality of life.
1. The Immune Win (The Mannick Trials)
For decades, doctors feared Rapamycin was purely "immunosuppressive" (due to its use in transplants to prevent rejection).
Mannick’s trials proved that at low, pulsed doses, it is actually immunomodulatory—it rejuvenates the immune system.
- The Data: In her landmark 2014 study (Science Translational Medicine), elderly adults given a rapamycin analog (everolimus) showed a 20% better antibody response to the flu vaccine compared to placebo.
- A 2018 follow-up showed patients actually got sick less often, with significantly reduced rates of respiratory tract infections.
- The Takeaway: Aging usually leads to immunosenescence (a tired immune system). This proves rapamycin can chemically "re-tune" an older immune system to fight like a younger one.
2. The Muscle Win (PEARL Trial, 2025)
The “Participatory Evaluation of Aging with Rapamycin for Longevity” (PEARL) study examined healthy older adults in a 48-week randomized, double-blind, placebo-controlled trial.
- The Data: Women taking 10mg of compounded rapamycin weekly saw significant improvements in lean tissue mass and self-reported pain. The 5mg group also reported improvements in emotional well-being and general health. Notably, this trial missed its primary endpoint (decreased visceral fat).
- The "Hidden" Insight: The study found that the compounded rapamycin has poor absorption (about 1/3 that of generic tablets), making the effective dose quite low (~3.3mg generic equivalent).
- And yet, it still produced a structural change in women (though not in men, likely because the dose was too low for their larger body mass).
- The Takeaway: Muscle loss (sarcopenia) and chronic pain are usually considered inevitable. This study suggests we can chemically preserve our metabolic engine, even at modest doses.
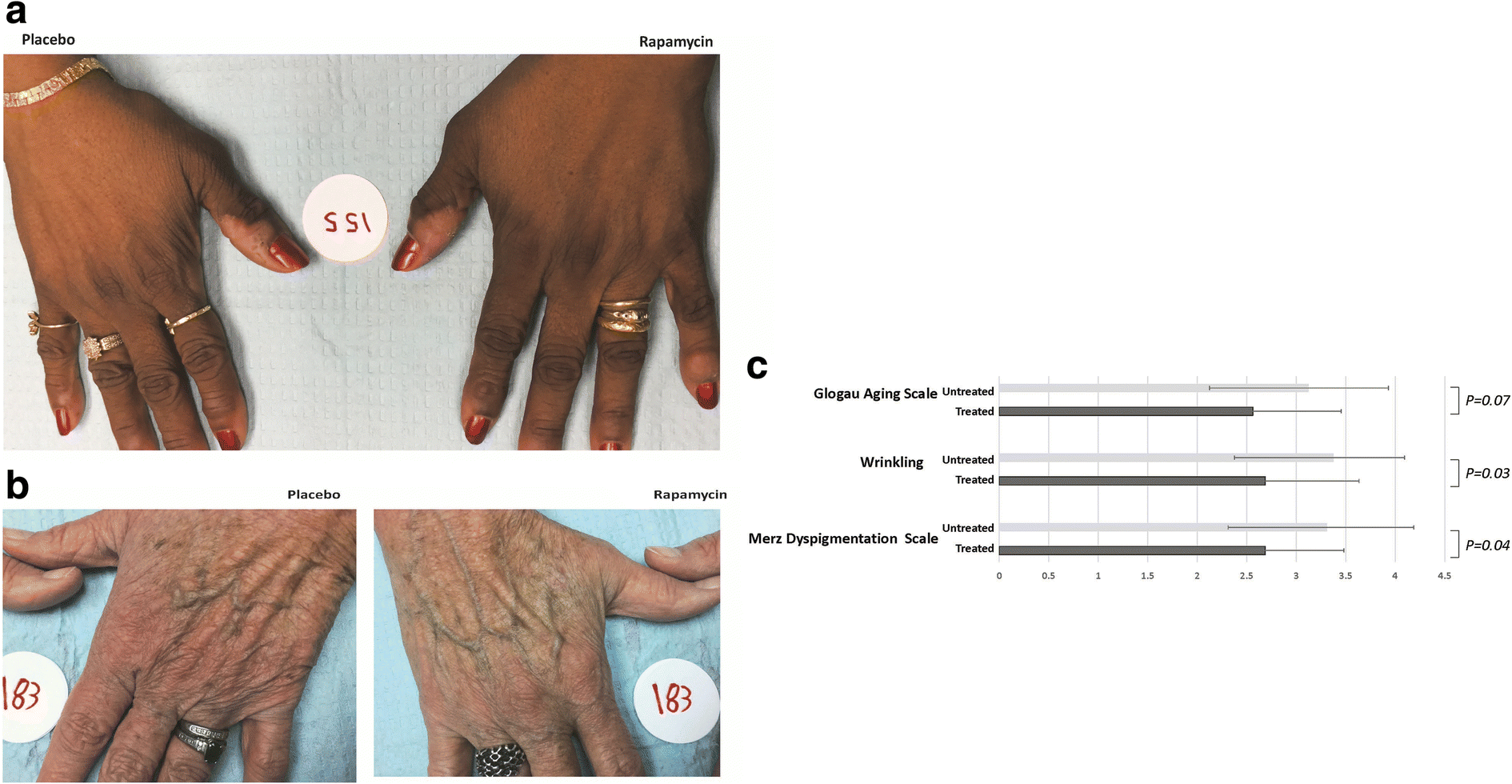
3. The Skin Win (The Drexel Study)
Skin is the most visible sign of aging. In 2019, researchers at Drexel University showed rapamycin's topical effects are more than just skin deep.
- The Data: After eight months, the rapamycin-treated hands showed significantly less p16 (a key marker of senescent "zombie cells") and more collagen VII.
- The Takeaway: This wasn't just cosmetic; it was structural. The drug cleared out the cellular junk and rebuilt the protein scaffolding.
4. The Ovarian Win (VIBRANT Trial)
While we often focus on heart or brain health, the ovaries are the “pacemaker” of female aging—they age faster than any other organ.
- The Data: Preliminary data from Columbia University’s VIBRANT trial suggests that weekly Rapamycin could delay ovarian aging by up to 20%.
- The Takeaway: By delaying menopause by up to 5 years, rapamycin preserves the hormonal environment that protects women’s bones, brains, and hearts.
5. The Energy Win (ME/CFS & Autophagy)
“Brain fog” and chronic fatigue are often dismissed as vague symptoms. A recent 2025 pilot study on ME/CFS (Chronic Fatigue Syndrome) gave us the mechanism.
- The Data: Patients on 6mg/week saw significant improvements in fatigue and post-exertional malaise.
- The Takeaway: The drug didn’t just “boost” energy; it restored autophagy (cellular cleanup) in neurons and flushed out the “cellular sludge” that was clogging the system.
6. The DNA Win (The Oxford Study, 2026)
And in 2026, a paper published in Aging Cell fundamentally shifted our understanding of Rapamycin.
- The Data: Researchers exposed human T-cells to DNA-damaging agents.The cells treated with Rapamycin had significantly lower DNA damage burdens and double the survival rate.
- In this trial's group of older adults, those taking rapamycin had significantly lower levels DNA damage and senescence.
- The Takeaway: We used to think Rapamycin just cleaned up the cell (autophagy). This proves it also protects the "instruction manual" itself—repairing and preventing damage to the DNA.
- There are also potential use cases for cancer patients and astronauts, who are exposed to higher levels of radiation.
📋 The Rapamycin for Longevity Protocol
Disclaimer: I am a doctor, but I am not your doctor. This protocol reflects my clinical practice and interpretation of the current data. Rapamycin is a potent immunomodulator. You should strictly work with a longevity-literate physician to evaluate your specific risks, particularly regarding lipids, glucose metabolism, and existing infections.Reading the studies is one thing; applying them to a living, breathing human is another.
In medicine, context is everything. Transplant patients take rapamycin daily. Their goal is immunosuppression—keeping the drug levels constantly high to prevent the body from rejecting a new organ.
In longevity, our goal is the exact opposite. We want immunorejuvenation.
To achieve this, we don't want a flat line; we want a pulse. We aim for a high peak to trigger autophagy and DNA repair (the "cleanup"), followed by a complete washout to allow for growth and recovery.
Here is the protocol I use in my clinic to achieve that signal:
1. The Safety On-Ramp
I never start a patient at a full dose. I typically start at 1mg or 2mg weekly.
- The Goal: We are testing for tolerance. The most common side effect is aphthous ulcers (mouth sores). While not dangerous, they are a sign that we need to pause, let them heal, and restart slower.
- The Caveat: Some practitioners prescribe daily micro-dosing. While valid in specific cancer contexts, the Mannick trials showed that weekly dosing produced a better immune response with significantly fewer side effects than daily dosing.
2. The Individual Targeted Dose
Over a period of 2–3 months, we slowly increase the dose. My target isn't a random number; it depends on Lean Body Mass.
- For Women: I typically target up to 6mg weekly.
- For Men: I typically target up to 10mg weekly.
Why the difference? It comes down to physics, not gender. Rapamycin is lipophilic (binds to fat and tissues), and its primary target (mTOR) is highly active in skeletal muscle. A 200lb male with high lean mass acts as a much larger "sink" for the drug than a 125lb female.
- If we under-dose a larger person, the drug gets diluted across their muscle mass and never hits the "peak" concentration needed to shut off mTOR and trigger that deep cellular cleanup.
- A 10mg dose for a larger male creates roughly the same physiological "shock" as a 6mg dose for a smaller female.
3. The Absorption Details
The dose means nothing if the delivery is wrong. Here are the three rules that make or break the protocol:
- The "Fat Multiplier": Rapamycin is poorly absorbed on an empty stomach. Taking it with a fatty meal (e.g., avocado, olive oil, yogurt) increases bioavailability by ~35%.
- Rule: Be consistent. If you take it with fat, always take it with fat. Switching between fasted and fed effectively changes your dose by nearly half.
- The "Grapefruit Effect": Never take Rapamycin with grapefruit juice or other strong CYP3A4 inhibitors (check existing medications).
- Risk: This can inhibit the enzyme that breaks down the drug, skyrocketing blood levels by 300%+ and turning a safe longevity pulse into a toxic overdose.
- The "Sick Day" Rule: Because Rapamycin modulates the immune system, I advise patients to skip their dose if they feel a cold coming on, have an active infection, or are scheduled for surgery. We want the immune system fully active for defense, not distracted by "cleanup mode."
Monitoring: What We Watch For
Rapamycin is not a "set it and forget it" drug. It requires active monitoring because it pushes on major metabolic levers. Here is what I track in my patients to ensure safety.
1. Subjective Side Effects (What You Feel)
- Aphthous Ulcers (Mouth Sores): The most common side effect (~15%). It is not dangerous, but it's a sign the dose is too high or escalating too fast.
- Fix: Pause dosing until healed, then restart at a lower dose.
- Bacterial Infections: While Rapamycin improves viral immunity (flu/COVID), it can slightly delay bacterial wound healing.
- Fix: Stop the protocol immediately if you have an active infection, need antibiotics, or have a surgery scheduled.
- Acne / Rash: A small percentage of users experience a mild, transient rash or acne flare-up as the immune system modulates skin flora.
2. Objective Biomarkers (What The Blood Shows)
- Lipids (LDL & Triglycerides): Rapamycin blocks the uptake of lipids into tissues (forcing the body to burn fat), which leaves more fat circulating in the blood.
- The Signal: We often see a mild rise in LDL or Triglycerides. This is usually benign, but if it spikes dramatically, we adjust the dose or add lipid-lowering therapy if the patient is particularly high-risk.
- Glucose & HbA1c: This is the most misunderstood marker. Rapamycin can cause "benevolent pseudo-diabetes."
- The Mechanism: The liver, sensing "starvation" (mTOR inhibition), pumps out glucose for fuel (gluconeogenesis). This raises fasting blood sugar, but the body remains insulin sensitive.
- The Watch-out: We differentiate this from true insulin resistance by checking fasting insulin. If glucose rises but insulin stays low, it is likely the drug working mechanistically. If both rise, the dose is too high (inhibiting mTORC2).
- Complete Blood Count (CBC): We monitor for anemia or low white blood cell counts (leukopenia), though this is rare with weekly pulsed dosing unless the user has a pre-existing (sometimes inherited) condition.
Rapamycin is a high potential longevity intervention, but it is far from being fully-proven. I do not actually prescribe it for the majority of my own patients; only to those who thoroughly understand the risk-benefit ratio and came to the decision after education.
⚡ Longevity Quick Hits
🧬 The New Hallmark: It’s Not the Trash, It’s the Factory We’ve spent a decade obsessed with autophagy (cleaning the cell’s waste), but a new Nature Cell Biology paper (Donahue et al., Feb 9) suggests we missed the upstream driver: ER-phagy. This is the process of remodeling the Endoplasmic Reticulum, or protein factory.
- The study shows that if the "protein factory" can’t remodel, the cell goes senescent regardless of how much you fast or take rapamycin. Expect longevity biotech to start designing "ER-shapers" like FAM134B.
🧠 Worrying About Aging...Is Aging You For the first time, researchers at NYU have linked "aging anxiety" directly to accelerated biological aging, specifically speeding up the DunedinPACE clock.
- The study took data from 726 women in the Midlife in the US (MIDUS) study.
- The data suggests a cruel feedback loop: if you are stressing about your biological age, you may be actively worsening it.
⚡ The "Living Drug" Pivot: Klotho Avant Technologies has a new "cell-in-a-box" encapsulation technology designed to deliver Klotho—the famous "anti-aging protein"—continuously into the bloodstream.
- We’ve known for years that Klotho overexpression extends lifespan (by ~30% in mice) and enhances cognition, but it’s a large, unstable protein with a terrible half-life. You can't put it in a pill.
- Instead of injecting the drug, you implant a shielded capsule of cells that manufacture the drug 24/7. It’s the same tech being used for Type 1 Diabetes (beta cell replacement), now finally successfully repurposed for longevity targets.
- If this holds up, "protein replacement therapy" for aging becomes a reality.
🫀 Until Next Week
Rapamycin is no longer just a cleanup drug. The evidence now spans six distinct human tissues — immune cells, muscle, skin, ovaries, neurons, and DNA itself.
That's not a lucky finding. That's a pattern.
But I still don't prescribe it to most of my patients. The data is compelling and accelerating, but we're early. The right candidates are the ones who've read the evidence, understand the trade-offs, and have a physician watching their bloodwork.
If that's you — bring this newsletter to your doctor. That's why I wrote it this way.
Next week: we'll cover a different type of longevity intervention. No prescriptions required — just shoes.
To your healthspan,
Hillary Lin, MD
Co-Founder & CEO
Follow me for more longevity insights: YouTube | LinkedIn | Instagram | TikTok
Want to turn your wellness brand into a full-service health destination? Learn about Care Core's platform or Get Started Here
Where to find me:
I'll be at the Integrative Healthcare Symposium in NYC – Feb 19-21. Let me know if you're there and we can sync up!
👱🏻♀️👩🏻🦰👩🏻👧🏽👧🏾 Livelong Women’s Health Summit – April 17-18, 2026, SF, CA. Delighted to join 50 other thought leaders in speaking on women's longevity! (Code HILLARY50 for $50 off)
Support us with your longevity purchases:
NeuroAgeTx is offering the most comprehensive and science-backed brain aging package to The Longevity Letter readers at up to 61% off (affiliate link here)
Timeline offers the patented Urolithin A for scientifically proven mitochondrial support via mitophagy.(Code CARECORE for 10% off).
GlycanAge measures your immune system's biological age, offering an easy way to detect "inflammaging" and recommend how to fix it.
ZBiotics is one of my favorite brands, because they offer two pro-longevity probiotics for when you *do* have a little fun (alcohol or sugar!). (Code CARECORE for 10% off.)